What’s working to expand behavioral healthcare access: 5 best practices


Just about everyone has a story about a mental health challenge or substance use disorder that is personal to them, whether a family member, close friend, or they themselves were affected. The pandemic heightened our awareness of both the need for behavioral health support and the difficulties that people can face in finding care. The good news is that progress is being made to expand access to care, although there is certainly more work to do.
When we surveyed employers in back in 2021 on their strategic priorities for their health programs, expanding access to behavioral healthcare was #1 among the nation’s largest employers (20,000 or more employers) and #2 among all large employers (500 or more employees). It remains in the top three today, and for good reason: Quality BH providers are in seriously short supply. According to the Health Resources and Services Administration, as of September 2023 there are 6,624 areas of the country -- with a total of 165 million residents – that currently face a shortage of mental health professionals. While employers can’t solve the provider shortage, they have taken action to expand access through their benefit programs. According to a Mercer survey, over the past 2-3 years 69% of large employers enhanced or expanded their EAP services and 42% added a supplemental network for virtual or in-person behavioral healthcare.
The impact of efforts to expand access to care
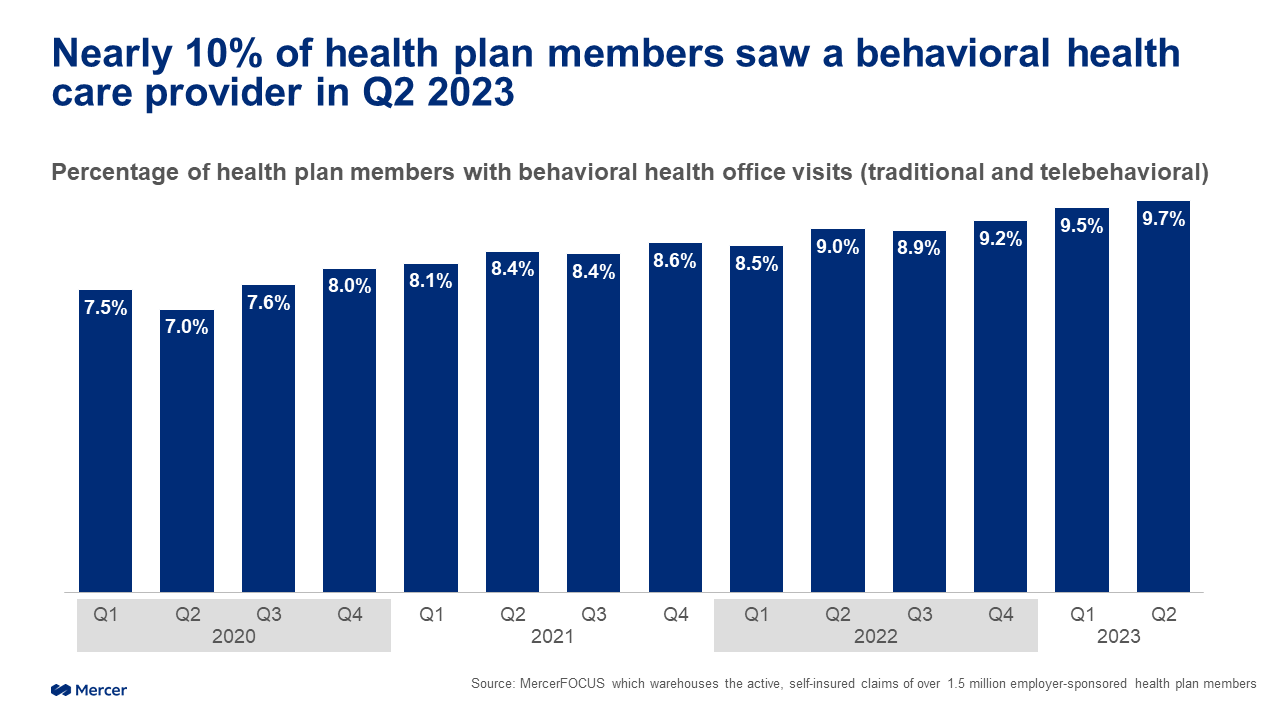
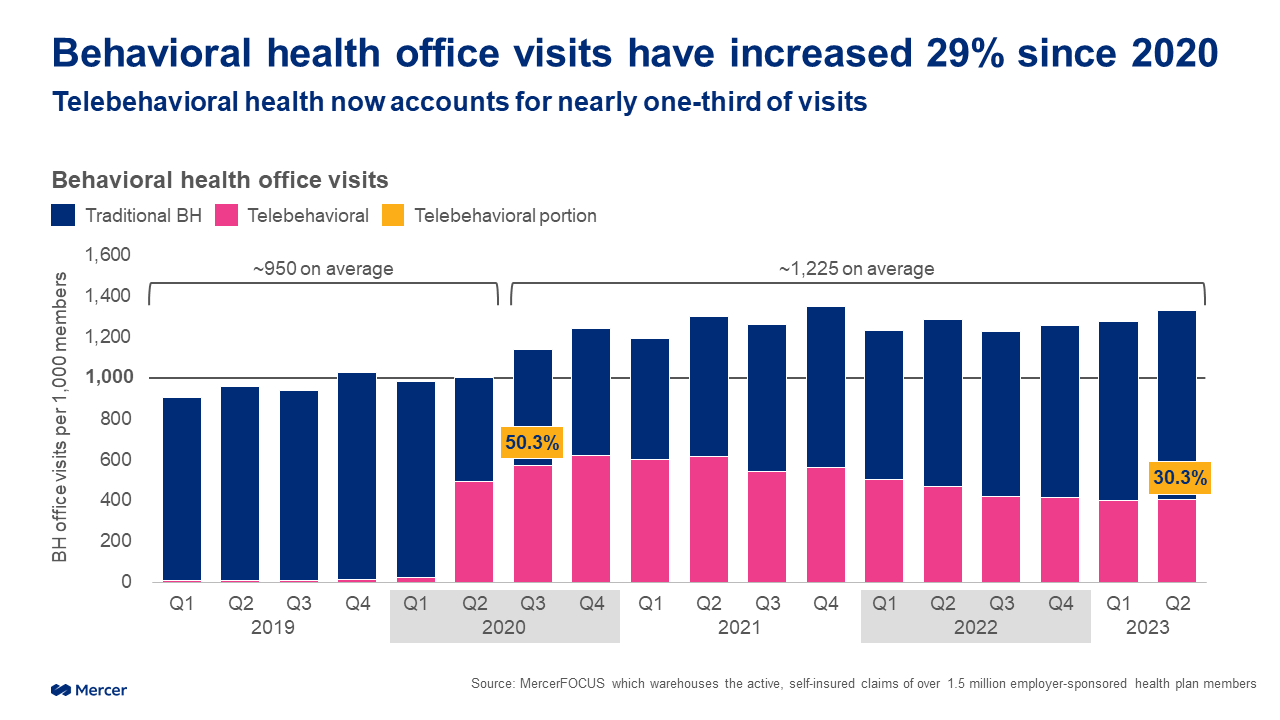
We also found that the total number of visits increased. Pre-pandemic, during 2019 and the first half of 2020, on average there were about 950 visits per 1,000 plan members each quarter. That jumped to an average of about 1,225 visits per 1,000 members each quarter after that.
Importantly, the data suggests that access to telebehavioral healthcare is likely the single biggest reason that more people have been able to get care and that the number of visits has increased. Virtual BH care was effectively non-existent prior to the pandemic. It spiked dramatically at the beginning of the pandemic, peaking at about 50% of all BH visits in Q3 2020. But while that percentage went down somewhat once people were able to safely resume in-person care, as you would expect, it has leveled over the past four quarters at a still substantial 30% of all BH visits. That could not have been predicted.
Five best practices for better BH access
Of course, it would be premature to declare victory. In Mercer’s Health on Demand survey, when we asked over 2,000 US workers whether it was easy to get quality mental healthcare, only 38% agreed that it was, while 40% said it was not easy (22% were not sure). The data also points to health equity problems: Workers with household income (HHI) at or below the median were much more likely to report difficulty in finding and accessing quality BH care (47%) than those with HHI above the median (34%). For those identifying with LGBTQ+, over half (53%) report difficulty in accessing BH care.
But over the past few years we have learned that employer actions can make a difference. Here are five best practices for improving access to BH care for your own population:
Add a virtual BH care network. Not only will members benefit from expanded access and greater convenience, they may save money as well. Virtual visits are typically less costly and avoid additional expenses associated with time off from work, travel, parking, and for some, childcare. More affordable care is more accessible care; consider lower cost-sharing to encourage use of the virtual network.
Enable patients to find a good provider match. Providing information about the providers’ background, expertise and lived experience has become so important to support the diverse needs of the population.
Make it as easy as possible. When someone is struggling with a BH condition or trying to support a family member in crisis, they shouldn’t have to navigate a complex process in order to access care. How can you make programs resources easier to find and access? Look for vendor partners and networks that provide triage services and will match the member with most appropriate type of provider – and help with scheduling so that members are not left to contact multiple providers to figure out who is available.
Help members become familiar with 988 and mobile crisis-response resources in the communities where they live. In many states, these programs were developed alongside Medicaid programs and have a proven track record. By intervening in acute situations in the field, mobile crisis-response teams decrease utilization of emergency departments and inpatient hospital admissions. Not only is this type of intervention cost-effective, it can help people in crisis avoid the long waits and sometimes traumatizing experience of being seen in an emergency room setting.
Address stigma with campaigns to encourage use of BH resources. Mental health issues are often stigmatized, which can make it difficult for people to seek help. Stigma can come from society, family, and friends, and be internalized as well. Keep in mind in crafting communications that different cultures may view mental health issues differently. Manager training can help in recognizing issues and steering people to resources.
Of course, these best practices cannot close all the gaps for those seeking treatment for mental health and substance use disorders. But there’s evidence that they have enabled employers to reach and support more people in need, and that’s a good foundation to build on.