New RxDC reporting instructions: Headaches or opportunities?





CMS released instructions for the third prescription drug data collection (RxDC) reports due June 1, 2024 – and they may cause plan sponsors to reconsider whether they need to make “plan level” submissions, instead of relying on their vendors to make “aggregate” submissions on their behalf. The good news is that the instructions largely mirror prior versions, so plan sponsors should be able to build off prior RxDC reporting efforts. However, for the first time, CMS plans to enforce the “aggregation restriction”—a provision in the 2021 regulations that CMS suspended for the first two reporting cycles. As explained below, the reinstated aggregation restriction may cause headaches for some plan sponsors, who find that they can no longer rely on their PBM’s aggregate submission of pharmacy data but must instead submit plan level data. Other plan sponsors may welcome the opportunity to do a plan level submission so they can obtain otherwise unavailable prescription drug data. As we’ll discuss, gaining access to this data may help fiduciaries to meet their obligations.
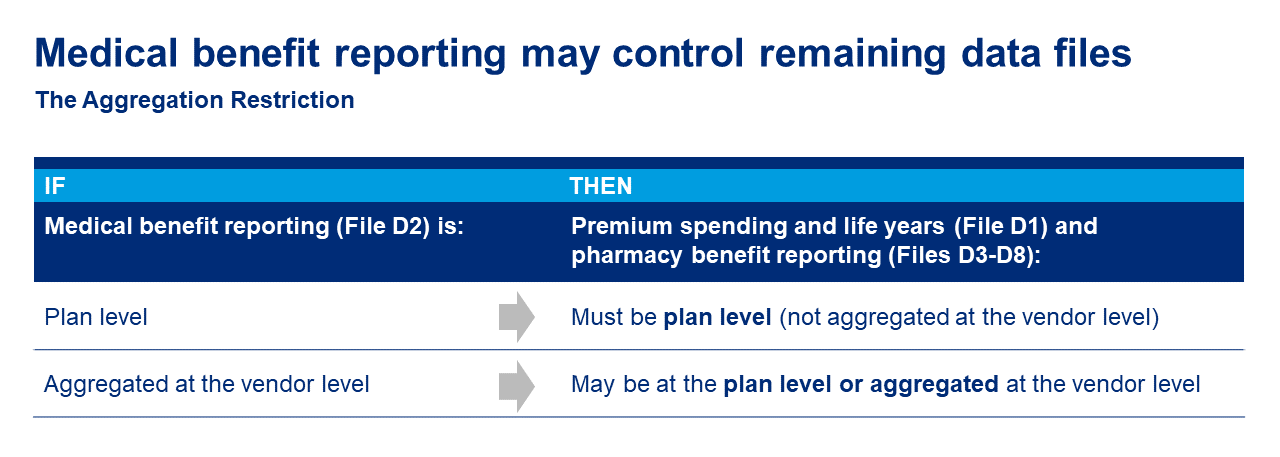
Refresher on the aggregation restriction
The aggregation restriction prohibits plans from having their vendors submit medical premium and life years data reported on file D1 and the pharmacy benefit data reported on files D3 through D8 “at a less granular level” than the medical benefit data (i.e., all healthcare spending other than the pharmacy benefit) reported on file D2. Under this complex rule, if the D2 file is submitted at the plan level, then files D1 and D3-D8 also must be submitted at the plan level. Importantly, the aggregation restriction works in one direction only – even if a plan sponsor submits pharmacy data at the plan level on the D3-D8 files, the plan can still rely on an aggregate TPA or insurer submission for the medical benefit D1 and D2 files. And if a plan’s TPA or insurer submits an aggregate D2 file, the plan can choose to how to submit its remaining D files—it can rely on aggregate vendor files, or it can submit one or more files at the plan level.
“Most granular” D2 controls
Many employers have multiple entities with information to report on the D2. This includes not only TPAs or insurance companies, but also other vendors for the health plan – for example, a behavioral health carve-out vendor or a fertility point solution might have reportable information not captured in the medical TPA’s data. The instructions state that the “most granular” D2 submitted on behalf of a plan will determine how the aggregation restriction applies to its D1 and D3-D8 files. As a result, if any one of a plan’s vendors has data for the D2 but won’t submit it as part of an aggregated file, the plan sponsor should ensure that all of the plan’s D2 data is submitted and also—new for the third reporting cycle—ensure that the plan’s remaining D files are submitted at the appropriate level (most likely, at the plan level).
How can RxDC help plan sponsors
The RxDC medical benefit files do not include new information for most employers. However, the pharmacy files include data that is not typically provided to plan sponsors including:
- PBM profit margin (spread)
- Drug level rebates for the top 25 drugs
- Manufacturer cost-sharing assistance
Employers have a unique opportunity to obtain this RxDC pharmacy data – specific to their plan – by submitting pharmacy benefit files at the plan level. PBMs apparently are not providing this data to employers when they submit aggregate files on a plan’s behalf. Significantly, it isn’t necessary to make the entire submission at the plan level – employers can continue to rely on their vendors’ aggregate medical benefit submissions but submit pharmacy files at the plan level to gain access to critical financial prescription drug data.
Group health plan fiduciaries have heightened concern about fiduciary risks for a variety of reasons. Plan level filing – and the pharmacy benefit data newly available as part of that filing – may help fiduciaries to meet their obligations.
Other changes
Additional changes for the third RxDC reporting cycle include:
- Additional data elements to report. New for this year, one of the pharmacy benefit files (the D6) asks for pharmacy enrollment information. Also, a group health plan’s plan list (P2) file must identify the types of carve-out benefits (i.e., pharmacy, medical, fertility, behavioral health). This information was optional last year.
- Simplifications to average monthly premium and premium equivalent calculations. Average monthly premiums will be simpler to calculate since they will no longer be reported on a per-member basis. Additionally, for average monthly premium paid by members, CMS clarifies that COBRA contributions and spousal and tobacco surcharges should be included. The instructions simplify the calculation of premium equivalents by removing restrictions on reporting on a cash basis. The instructions also describe how Employee Group Waiver Plan (EGWP) premiums or premium equivalents should be reported.
Time to get started
The new instructions do not provide good faith relief for the third RxDC submission, nor do they extend the deadline because June 1, 2024 falls on a Saturday. Some vendors are already requesting information from plan sponsors, and with very short turnaround times. Plan sponsors should begin to work on their reporting strategy now, starting with identifying all vendors with required data, confirming the reporting entities for every data file, and responding to all vendor surveys by the specified deadline. But keep the big picture in mind—beyond the administrative burdens, self-reporting plan-level RxDC pharmacy files may provide plan sponsors with valuable pharmacy benefit data.