Designing fiscally viable coverage of GLP-1 weight-loss drugs



The obesity epidemic may be the worst health crisis facing this country, given the number of people affected, the associated health risks, and the impact on health care spending. At last there is a promising treatment for this chronic disease – FDA-approved GLP-1 Anti-Obesity Medication (AOM) such as Wegovy and Saxenda – but the cost implications are concerning.
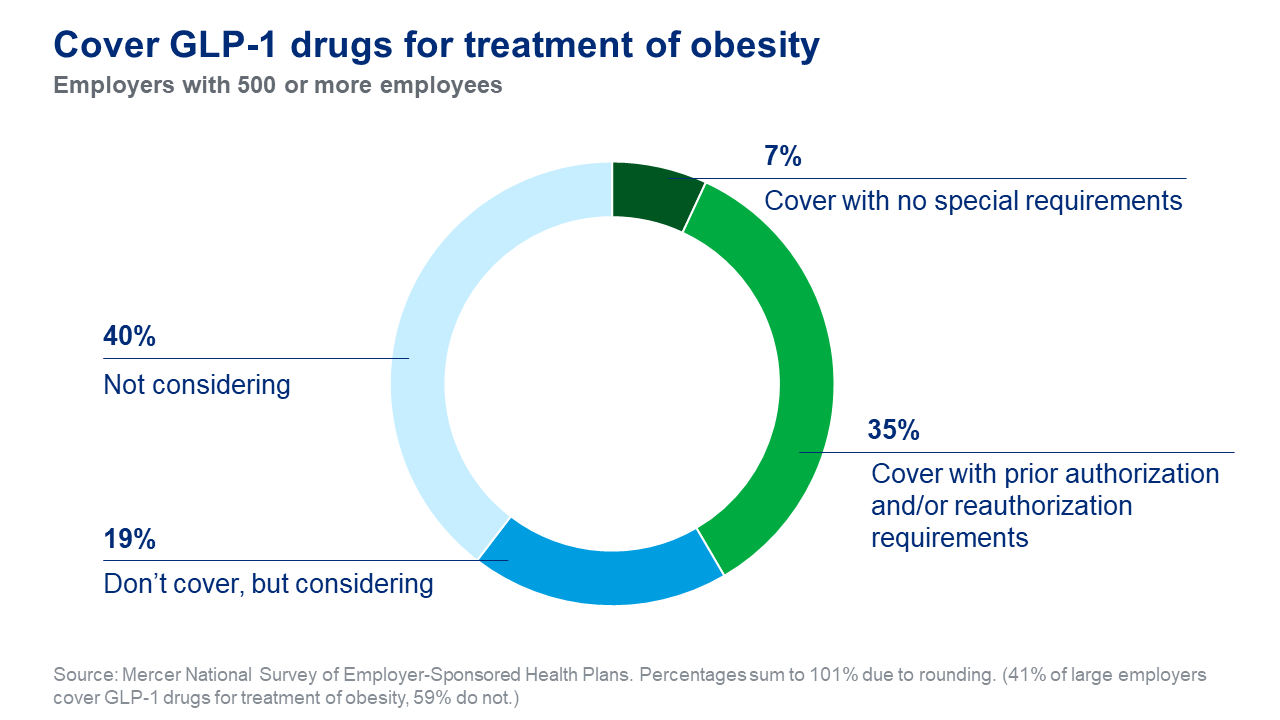
The combination of the very high price of these drugs – typically about $1,000 per month per patient – plus a relatively large number of patients who may benefit from them can result in a substantial net new cost to a health plan, potentially more than many employers – or the employees who share the cost of coverage – can afford. It’s not surprising, then, that results from Mercer’s National Survey of Employer-Sponsored Health Plans 2023 show that fewer than half of large employers (42% of those with 500 or more employees) currently cover GLP-1 medications for treatment of obesity, although another 19% say they are considering it.
But while GLP-1 coverage for obesity treatment is the focus of the clinical and financial assessments and decisions for coverage, the clinical reality is that GLP-1 medications are also recommended for certain high-risk type 2 diabetes (T2DM). Clinically, a majority of T2DM cases are due to obesity. It’s likely that a high percentage of those with obesity will progress to T2DM – and ultimately end up on a GLP-1 drug anyway. So, the broader question is whether it is both clinically and economically better to aggressively treat certain high-risk obese patients sooner, or risk downstream cost and clinical complexity later.
The decision to cover or not cover GLP-1 obesity treatment options for employees and family members requires employers to weigh the clinical and financial implications. But decision-making is complicated by the lack of key quantifications and data to understand the current state of their employees’ medical situations.
When healthcare providers approach the treatment of obesity, considered a chronic disease, they will follow the latest treatment guidelines, which include considering GLP-1 AOMs for certain high-risk obese individuals. Who are in the risk group that potentially may be considered for GLP-1 treatment? Employers can analyze claims data and possibly health risk assessment data to estimate the prevalence of obesity, which has historically been grossly undercounted. Another approach is to quantify current GLP-1 utilization and cost (including use for treating T2DM). Such an analysis could include:
- Quantifying utilization and cost and assessing clinical reasons for utilization.
- Examining adherence and/or discontinuation rates (side effects can cause discontinuation).
- Assessing current coverage policy and process, including prescription prior authorization.
- Analyzing prescribing and utilization.
Forging a path to fiscally sustainable coverage of AOM
Should you choose to cover GLP-1 AOMs, what are ways to ensure appropriate utilization, optimize outcomes, and drive towards some degree of quantifiable positive cost and benefit and added value?
In cases where an employer is providing plan coverage for GLP-1 medications for obesity, there are risks and potential unforeseen consequences if the coverage doesn’t have a defined plan structure and a managed process for treatment. There have already been reports of organizations reversing previous coverage of GLP-1 for obesity due to high utilization and extremely high costs to the plan.
The high cost of GLP-1 plus the risk of inappropriate or unnecessary prescriptions requires GLP-1 coverage to be a structured process with checks and balances to ensure necessary and effective prescribing and avoid side effects that can result in early discontinuation. Supply shortages of Wegovy and others may impact successful treatment. Guidelines typically call for engagement with intensive lifestyle interventions to address key influencers of cardiometabolic health and optimize weight loss and physiological improvement. There is the possibility of switching to lower cost anti-obesity medications, or even tapering off AOM and sustaining the improved health state with ongoing lifestyle changes.
It will be interesting to see where healthcare organizations land on some of these questions, since many are in the unique position of both sponsoring health coverage and providing actual care to their employees. For this reason, they may need to move more quickly than other employers to determine a coverage approach. While their choices may help to inform the decision-making of plan sponsors in other industries, ultimately all employers will need to weigh the clinical and financial issues to ensure their benefit design reflects their philosophy, program objectives and fiscal reality.