Weight-loss medications: Q&A with Mercer’s pharmacy team


Employers have had a busy year trying to keep up with the latest prescription drug headlines: multimillion-dollar therapies, dropping insulin prices, drug shortages, new biosimilars, over-the-counter contraceptives, challenges to vaccines, state PBM legislation, and more. Of all this breaking news, we’ve found employers most want to discuss the use of GLP-1s to manage weight loss. Below, members of Mercer’s pharmacy practice answer employers’ most urgent questions on GLP-1s – why they have become so popular, how to pay for them, and what they mean for the future.
Why is there such increased attention on obesity and the use of GLP-1s to lose weight?
Sherry Welliver, PharmD: GLP-1s, like Ozempic, have been on the market for years to treat Type 2 diabetes. They're very effective at managing blood glucose, but they're also effective at weight loss. If you think about the fact that just over 60% of US adults who are diabetic are also obese, GLP-1s can be a great option for these patients because they need help with both weight loss and managing Type 2 diabetes.
Social media posts on TikTok and Saturday Night Live skits about Ozempic have introduced GLP-1s to Americans interested in a fast and easy way to lose weight. As a result of these and other pop culture references, and because GLP-1s are often covered by insurance plans to treat diabetes, we're seeing an increase in off-label use for weight loss.
What’s happening with GLP-1 utilization?
Jon Lewis, FSA, MAAA, MercerRx Financial Leader: The utilization of GLP-1s in 2023 is quite different than in 2022. It is the number one driver of non-specialty pharmacy trend right now. For years, we've been talking about specialty pharmacy becoming a bigger and bigger percentage of overall pharmacy costs. But because of GLP-1s, we may see a plateau or a potential decrease in overall specialty pharmacy as a percentage of pharmacy costs.
The other thing we're seeing with GLP-1s is a lot of volatility. We're seeing some employer plans with GLP-1 costs as low as $5 per-member-per-month and others as high as $40 per-member-per-month.
It’s also important to consider that females are about four times more likely to take GLP-1s than males. And we are seeing high discontinuation rates. In some cases, we’re seeing 50% discontinuation rates within five to six months. You would think discontinuation rates should help trend and it does, but at this point the number of new members filling GLP-1 prescriptions is exceeding the discontinuation rates. This new demand is causing upward pressure on costs.
What are plan sponsors doing to manage the costs and maximize the value? Will their strategies change over the next 12 months?
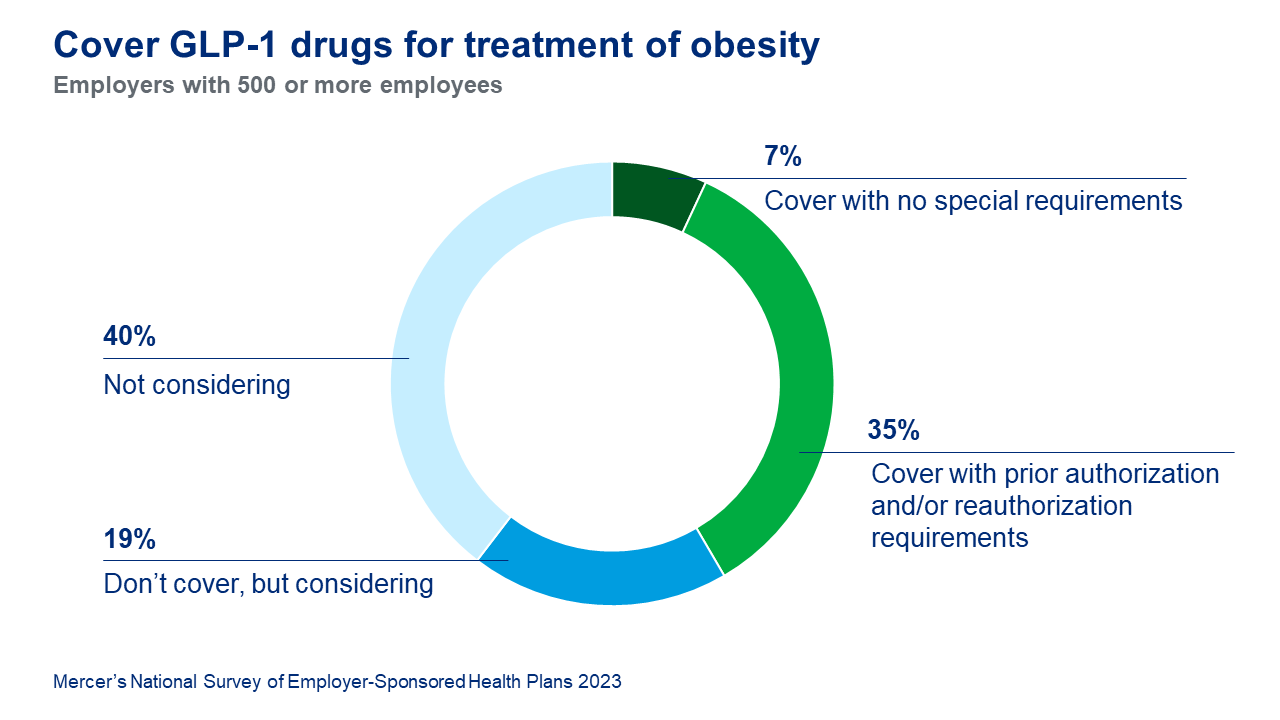
Sherry Welliver: Of the 42% of large employers covering GLP-1 drugs for treatment of obesity, the great majority require prior authorization.
Prior authorization criteria often have requirements tied to body mass index and nutritional coaching. With the increase in utilization and costs, we may see more aggressive criteria like longer waiting periods, more prescriptive coaching and wellness requirements, and even limits on who can prescribe GLP-1s.
We also expect more formulary strategies will come into play. There are some GLP-1s and innovative products in the pipeline that will create more competition in the formulary, but right now we need to monitor supply shortages due to high demand.
Additionally, we are seeing some vendors put in what we call smart edits to decrease off-label use – taking GLP-1s indicated for diabetes for weight loss. This approach seems to be helping manage off- label use.
Do these medications have an ROI? When might plan sponsors expect to see benefits from treating obesity as a chronic disease?
Jon Lewis: These medications represent a big investment. While everyone talks about the high list prices, it is worth noting something fairly unique here. We do have manufacturer competition which means rebates are playing a role and should be monitored.
In general though, we are looking at somewhere between three to five years before you start to realize any savings. Those who are at higher risk – for example, people with a higher BMI – are likely to produce more savings. With that said, changing eligibility to a narrower BMI does have a rebate impact and should be incorporated into any weight loss strategy.
But these drugs are costly. You would have to have someone who is on the drug long enough to achieve the weight loss, still be employed, and still be maintaining that weight loss over the course of three to five years to see an ROI or some form of savings.
How should plan sponsors be thinking about GLP-1 coverage moving into 2024?
Alysha Fluno, PharmD, MBA, National Pharmacy Practice Leader: There isn’t a day where our MercerRx team isn’t talking with employers about GLP-1s – whether they are covering them today or not. This topic is top of mind for everybody.
For those employers who are currently covering GLP-1s, if you can continue to withstand the volatility in supply and manage the expense, we recommend continuing coverage, as discontinuing it could be disruptive and confusing to members who are currently responding well to therapy.
If the cost of continuing coverage is simply too onerous, we recommend re-evaluating your program design by tightening approval and continuation criteria or, possibly, evaluating new coverage options through the PBMs or point solutions. The market will evolve significantly in the next three to six months as new drugs and programs enter the market.
For the 59% of large employers who are not covering obesity medications today, unless you're getting a lot of pressure from members, the best thing to do is to wait and see. There are three GLP-1 drugs FDA-approved for obesity: Wegovy, Saxenda, and now Eli Lilly’s Zepbound, although it will take some time for this new product to be available in the market. We anticipate that due to current supply issues with Wegovy, many PBMs will place both of these products on their formularies. We’re hopeful some of the supply shortages will begin to ease in the coming months. If you can wait, we think there is a possibility that the volatility will level out in the short-term and the drug supply will achieve a steady state.
Listen to our full conversation about GLP-1s and other prescription drug topics here.